It always starts with just one: one opiate; one drink; one injection. However, the end result always varies. Some only try it once. For the most unfortunate, the substance becomes their life. The hunt for the drug becomes all-encompassing, consuming almost every aspect of the addict’s life. But why? Why are some people addicts and some merely experimenters?
'Why Can't You Just Stop?'
For years, researchers have asked this question. Multiple theories have been used to explain this issue, yet most of the theories have been proven incorrect for various reasons. What is agreed upon by almost every researcher is that the desire to obtain the drug is more of a motivator than actually wanting to take the drug. In 2005, Peter Kalivas and Nora Volkow published their article “The Neural Basis of Addiction: A Pathology of Motivation and Choice” in The American Journal of Psychiatry in which they discussed this point:
…conditioned stimuli predicting the event continue to trigger release of dopamine. Therefore, in most natural situations where learned associations accompany a repeatedly encountered motivational event, dopamine will likely be released as part of the overall experience. …Although not an obligatory event, dopamine is released into the core in response to stimuli predicting a rewarding event and likely modulates the expression of adaptive behaviors.
Our brains are structured in such a manner that if dopamine is released because of an event, the cellular structure of the brain will initiate adaptive behavioral responses in reaction to the event. Therefore, the brain will later associate the drug with that release of dopamine. Obtaining the drug becomes as much, if not more, of a motivational force because of this release than actually taking the drug.
'Why Can't You Just Stop?'
For years, researchers have asked this question. Multiple theories have been used to explain this issue, yet most of the theories have been proven incorrect for various reasons. What is agreed upon by almost every researcher is that the desire to obtain the drug is more of a motivator than actually wanting to take the drug. In 2005, Peter Kalivas and Nora Volkow published their article “The Neural Basis of Addiction: A Pathology of Motivation and Choice” in The American Journal of Psychiatry in which they discussed this point:
…conditioned stimuli predicting the event continue to trigger release of dopamine. Therefore, in most natural situations where learned associations accompany a repeatedly encountered motivational event, dopamine will likely be released as part of the overall experience. …Although not an obligatory event, dopamine is released into the core in response to stimuli predicting a rewarding event and likely modulates the expression of adaptive behaviors.
Our brains are structured in such a manner that if dopamine is released because of an event, the cellular structure of the brain will initiate adaptive behavioral responses in reaction to the event. Therefore, the brain will later associate the drug with that release of dopamine. Obtaining the drug becomes as much, if not more, of a motivational force because of this release than actually taking the drug.
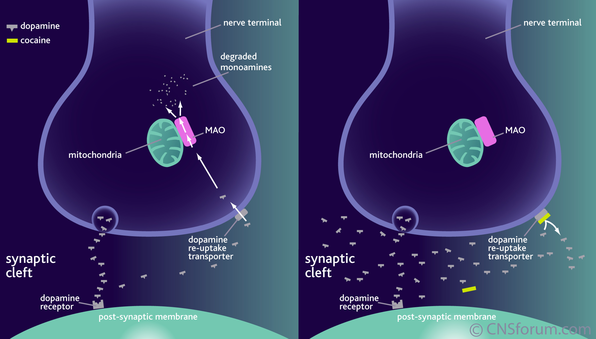 Dopamine synaptic cleft; normal vs. drugs
Dopamine synaptic cleft; normal vs. drugs
Theories of Enforcement
Two other theories are supported by the behaviorist model produced by B.F. Skinner, which states that behavior that is either positively or negatively reinforced increases with each reinforcement. Positive reinforcers reward the act, while negative reinforcers remove aversive stimuli.
For those who advocate these theories, the positive reinforcement is a result of the euphoria and pleasure one feels after administering a drug. Unfortunately, what this theory must then assume is a causal relationship between wanting drugs and liking drugs. Upon asking one patient at Brentwood Meadows why he first drank, he said, “I wanted to know what it felt like, ya know?” Another patient quickly, without hesitation, answered, “I wanted to be somewhere else, feel something else, just…be someone else.” These answers may support the positive reinforcement model at first glance. However, Terry E. Robinson and Kent C. Berridge explain that “if addicts craved drugs in proportion to their ability to produce pleasure, then craving late in addiction ought not be stronger than craving after the initial drug experience – but of course that is not the case.” The reasoning behind this statement is the way in which the brain functions when on a substance for a prolonged period of time.
In a normal brain, dopamine is released into the synapse. After this impulse, the remaining dopamine is taken back into the original cell and stored for future use. This prevents too much dopamine from being used, which can result in a change in the way in which neurotransmitters are transmitted. After use of a substance, the reuptake of dopamine is inhibited, meaning the extra dopamine is metabolized and excreted before it could be stored for future use. This calls for the dopamine enzymes to work harder than before, but they will not release the same amount of dopamine as they did on the initial use. Continued use is likely to result in dopamine depletion (Dackis et al 1985). Put simpler, because the amount of dopamine released after prolonged use is less than the initial use, the pleasure obtained from use is less than the initial use as well. Therefore, the positive reinforcement theory is not a viable explanation for addiction.
The negative reinforcement theory claims that addicts continue use to avoid withdrawal symptoms, which may include headaches, nausea, fatigue, anxiety, insomnia, depression, and difficulty breathing varying from drug to drug and person to person. What this theory lacks is support for drugs that can be highly addictive yet produce no withdrawal syndrome (psychostimulants). On the other hand, some drugs such as some tricyclic antidepressants show no sign of addiction yet produce tolerance and withdrawal syndromes (Robinson et al 2000).
Two other theories are supported by the behaviorist model produced by B.F. Skinner, which states that behavior that is either positively or negatively reinforced increases with each reinforcement. Positive reinforcers reward the act, while negative reinforcers remove aversive stimuli.
For those who advocate these theories, the positive reinforcement is a result of the euphoria and pleasure one feels after administering a drug. Unfortunately, what this theory must then assume is a causal relationship between wanting drugs and liking drugs. Upon asking one patient at Brentwood Meadows why he first drank, he said, “I wanted to know what it felt like, ya know?” Another patient quickly, without hesitation, answered, “I wanted to be somewhere else, feel something else, just…be someone else.” These answers may support the positive reinforcement model at first glance. However, Terry E. Robinson and Kent C. Berridge explain that “if addicts craved drugs in proportion to their ability to produce pleasure, then craving late in addiction ought not be stronger than craving after the initial drug experience – but of course that is not the case.” The reasoning behind this statement is the way in which the brain functions when on a substance for a prolonged period of time.
In a normal brain, dopamine is released into the synapse. After this impulse, the remaining dopamine is taken back into the original cell and stored for future use. This prevents too much dopamine from being used, which can result in a change in the way in which neurotransmitters are transmitted. After use of a substance, the reuptake of dopamine is inhibited, meaning the extra dopamine is metabolized and excreted before it could be stored for future use. This calls for the dopamine enzymes to work harder than before, but they will not release the same amount of dopamine as they did on the initial use. Continued use is likely to result in dopamine depletion (Dackis et al 1985). Put simpler, because the amount of dopamine released after prolonged use is less than the initial use, the pleasure obtained from use is less than the initial use as well. Therefore, the positive reinforcement theory is not a viable explanation for addiction.
The negative reinforcement theory claims that addicts continue use to avoid withdrawal symptoms, which may include headaches, nausea, fatigue, anxiety, insomnia, depression, and difficulty breathing varying from drug to drug and person to person. What this theory lacks is support for drugs that can be highly addictive yet produce no withdrawal syndrome (psychostimulants). On the other hand, some drugs such as some tricyclic antidepressants show no sign of addiction yet produce tolerance and withdrawal syndromes (Robinson et al 2000).
 Book written by Dr. Carl Hart
Book written by Dr. Carl Hart
Social Theories
In an article in The New York Times, John Tierney examined the choices that those addicted to crack made in an experiment by Dr. John Hart from Columbia University. Dr. Hart’s experiment was based on experiences from his childhood. His family, along with many in his neighborhood, was torn apart. He notes, however, that the crack addiction came after the families fell apart. He observes other situations in which a person only became a crack addict after other negative circumstances in his or her life. He writes “his cousins became destitute crack addicts living in a shed, but they’d dropped out of school and had been unemployed long before crack came along.”
For his experiment, Dr. Hart offered crack addicts a chance to make $950 while smoking crack and living in a hospital ward for several weeks. When each day began, the participants were blindfolded so as to not be able to see the size and administered an amount of crack. Each dose varied daily. Throughout the day, the participant could either smoke that same amount or choose to take the $5 reward. Typically, with a large dose, the participant would smoke. However, when it was a smaller dose, they chose the reward. In a second experiment, Dr. Hart increased the money to $20. Every addict chose the money.
These experiments revealed, according to Dr. Hart, that “if you’re living in a poor neighborhood deprived of options, there’s a certain rationality to keep taking a drug that will give you some temporary pleasure.” A psychologist at the University of Kentucky agreed, saying “They can stop using drugs when provided with alternative reinforcers.” Dr. Carl Nutt, a professor of neuropyshcopharmacology also agreed adding “Addiction always has a social element, and this is magnified in societies with little in the way of work or other ways to find fulfillment.”
In an article in The New York Times, John Tierney examined the choices that those addicted to crack made in an experiment by Dr. John Hart from Columbia University. Dr. Hart’s experiment was based on experiences from his childhood. His family, along with many in his neighborhood, was torn apart. He notes, however, that the crack addiction came after the families fell apart. He observes other situations in which a person only became a crack addict after other negative circumstances in his or her life. He writes “his cousins became destitute crack addicts living in a shed, but they’d dropped out of school and had been unemployed long before crack came along.”
For his experiment, Dr. Hart offered crack addicts a chance to make $950 while smoking crack and living in a hospital ward for several weeks. When each day began, the participants were blindfolded so as to not be able to see the size and administered an amount of crack. Each dose varied daily. Throughout the day, the participant could either smoke that same amount or choose to take the $5 reward. Typically, with a large dose, the participant would smoke. However, when it was a smaller dose, they chose the reward. In a second experiment, Dr. Hart increased the money to $20. Every addict chose the money.
These experiments revealed, according to Dr. Hart, that “if you’re living in a poor neighborhood deprived of options, there’s a certain rationality to keep taking a drug that will give you some temporary pleasure.” A psychologist at the University of Kentucky agreed, saying “They can stop using drugs when provided with alternative reinforcers.” Dr. Carl Nutt, a professor of neuropyshcopharmacology also agreed adding “Addiction always has a social element, and this is magnified in societies with little in the way of work or other ways to find fulfillment.”
 Wanda: Director of Quality/Nursing
Wanda: Director of Quality/Nursing
Other Theories
The Director of Quality, Wanda - who aslo serves as the Director of Nursing - at Brentwood Meadows noted that there is a “genetic predisposition” for addiction and that each person’s predisposition may differ. For example, about 50% of people have a genetic predisposition for an addiction to nicotine. She went on to say that those with a genetic predisposition have a different brain structure than normal. Because of this, “an alcoholic’s brain acts abnormally compared to someone who is simply a social drinker. An alcohol abuser feels that they have to have a drink to live. A social drinker has a drink every now and then. Unfortunately, an alcoholic feels the desire to drink in order to cope with every problem he or she faces in the daily routine.”
While many theories exist, one thing is clear: the structure of the brain changes. It is never an issue of “just stop using the drug.” The chemicals in the brain, mostly dopamine, can no longer function normally once addiction has begun, and thus, without help of some form, the addict may never be able to separate from the addiction and its physical and psychological effects.
The Director of Quality, Wanda - who aslo serves as the Director of Nursing - at Brentwood Meadows noted that there is a “genetic predisposition” for addiction and that each person’s predisposition may differ. For example, about 50% of people have a genetic predisposition for an addiction to nicotine. She went on to say that those with a genetic predisposition have a different brain structure than normal. Because of this, “an alcoholic’s brain acts abnormally compared to someone who is simply a social drinker. An alcohol abuser feels that they have to have a drink to live. A social drinker has a drink every now and then. Unfortunately, an alcoholic feels the desire to drink in order to cope with every problem he or she faces in the daily routine.”
While many theories exist, one thing is clear: the structure of the brain changes. It is never an issue of “just stop using the drug.” The chemicals in the brain, mostly dopamine, can no longer function normally once addiction has begun, and thus, without help of some form, the addict may never be able to separate from the addiction and its physical and psychological effects.
